Medication Adherence
The Basic Idea
In the realm of healthcare, adherence is the collaborative, active, and voluntary engagement of patients with a course of action agreed upon by them and their medical provider, all to produce a positive therapeutic result.1
Medication adherence, then, is the autonomous choice by a patient to stick to a plan of prescription medications created by their doctors. Many factors influence medication adherence, including, but not limited to:
- Social support
- High costs
- Low health literacy
- Depression2
- Level of income and one’s socioeconomic status3–5
Medication nonadherence can be broken down into two groups:
- Primary nonadherence: The medication isn’t filled by the pharmacy or picked up by the patient
- Secondary nonadherence: A patient, over time, starts to miss doses, prematurely stops the therapeutic course of action, or takes incorrect doses.6
The consequences of not following a medication regimen can be immense and lead to poor health outcomes like high patient morbidity or mortality.2 In addition to consequences to one’s health, medication nonadherence has significant public costs: in 2014, the Centers for Disease Control and Prevention (CDC) calculated that medication nonadherence among those with chronic diseases costs $300 billion USD each year in avoidable costs.7
At a more macro level, nonadherence also results in higher costs for individuals. For example, those with cardiac disease who stick to their therapeutic strategies spend on average $8,881 less for medical needs per year than their non-adhering counterparts.5
Theory, meet practice
TDL is an applied research consultancy. In our work, we leverage the insights of diverse fields—from psychology and economics to machine learning and behavioral data science—to sculpt targeted solutions to nuanced problems.
Contemporary Context
The increasing cost of medication means it can be difficult to adhere to regular medication schedules.
If a patient is struggling to pay for rent, food, their children’s needs, and their own medicine, they may choose nonadherence as a way to prioritize their family’s well being.
Between March 2020 and March 2022, prescription medication prices grew by almost 2%.8 Since 2014, prices have grown by an astronomical 35%.8 In fact, while inflation and other variables have caused an increase in most medical goods and services, the cost of prescription drugs have grown the most.
To lower medication costs, individuals may opt to skip doses, purchase medicines in other countries, or use alternative therapies.2 An estimated 8% of American adults don’t take their medicines as prescribed; this is particularly true for people between 18 and 64, and those who have incomes below the federal poverty level.9
To make matters worse, the majority of doctors often aren’t aware of the cost of the medications they prescribe10 and choose to prescribe expensive brand-name medications,11 even when generic medications will do.
To boost medication adherence, a promising direction is supporting policies that lower the cost of prescription medications - so patients are not forced to choose between making rent and taking medicine.

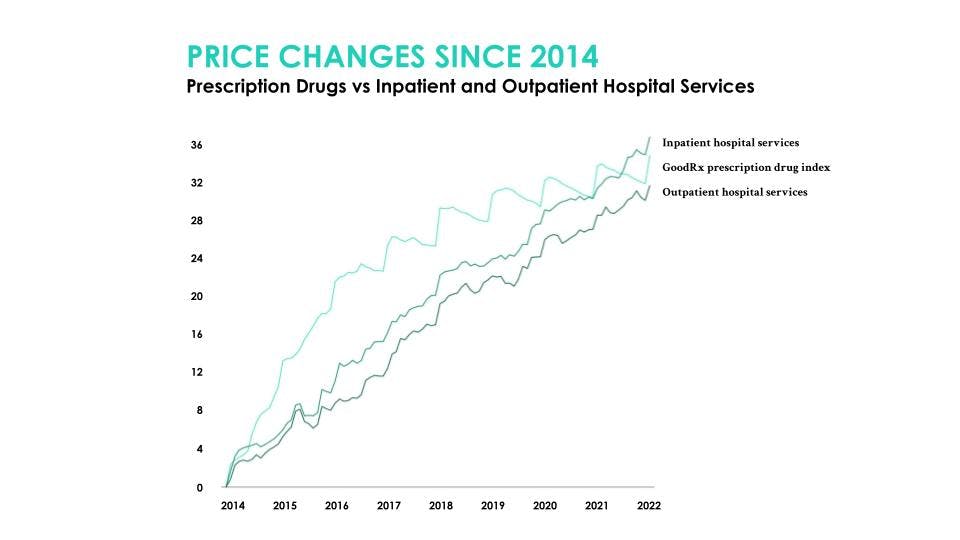
A graphical representation from GoodRx of the increases in inpatient and outpatient services and prescription drugs between 2014 and 2022.
The Behavioral Science
One way to boost medication adherence is to incentivize it. Incentivization is the act of attaching a reward to a behavior, or alternatively, threatening a negative consequence for not doing that behavior.
An incentive for medication adherence might look like having patients fill out a form each day they take their medications, and if they take it everyday for a month, they receive a voucher.
It’s important that incentives don’t demotivate patients from adhering to their medication plan - otherwise known as crowding out incentives.
Since incentives by nature shift motivation from intrinsic factors (internal rewards, e.g. maintaining health) to extrinsic factors (external rewards, e.g. vouchers), rewards like vouchers may backfire once they are no longer in use. By contrast, if a patient was never introduced to an external motivator, their intrinsic motivation would likely remain constant - no expectation for external rewards means our internal rewards are sufficient to continue the behavior.
Case Study
According to the World Health Organization, over 1.5 million people across the world live with hearing loss.12 In the United States, only 14.2% of those with hearing loss aged 50 years or older wore hearing aids between 1999 through 2006.13
Behavioral barriers drive this statistic more than cost or accessibility. To address this, Nessa, a leading provider of hearing aids in Southeast Asia, reached out to The Decision Lab to identify the specific behavioral roadblocks affecting the adherence of hearing aids usage.
Upon conducting an extensive literature review and analyzing a mock audiologist appointment, we were able to create a system that could identify behavioral roadblocks on a patient-to-patient basis. Using this patient-centered approach led to 270% higher adoption rates compared to the baseline.
You can read more about this case study here.
Citations
1. Ho, P. M., Bryson, C. L., & Rumsfeld, J. S. (2009). Medication Adherence. Circulation, 119(23), 3028–3035. https://doi.org/10.1161/CIRCULATIONAHA.108.768986
2. Piña, I. L., Di Palo, K. E., Brown, M. T., Choudhry, N. K., Cvengros, J., Whalen, D., Whitsel, L. P., & Johnson, J. (2021). Medication adherence: Importance, issues and policy: A policy statement from the American Heart Association. Progress in Cardiovascular Diseases, 64, 111–120. https://doi.org/10.1016/j.pcad.2020.08.003
3. Bowry, A. D. K., Shrank, W. H., Lee, J. L., Stedman, M., & Choudhry, N. K. (2011). A Systematic Review of Adherence to Cardiovascular Medications in Resource-Limited Settings. Journal of General Internal Medicine, 26(12), 1479–1491. https://doi.org/10.1007/s11606-011-1825-3
4. Mishra, S. I., Gioia, D., Childress, S., Barnet, B., & Webster, R. L. (2011). Adherence to Medication Regimens among Low-Income Patients with Multiple Comorbid Chronic Conditions. Health & Social Work, 36(4), 249–258. https://doi.org/10.1093/hsw/36.4.249
5. Roebuck, M. C., Liberman, J. N., Gemmill-Toyama, M., & Brennan, T. A. (2011). Medication Adherence Leads To Lower Health Care Use And Costs Despite Increased Drug Spending. Health Affairs, 30(1), 91–99. https://doi.org/10.1377/hlthaff.2009.1087
6. Lee, J. S., Joyce, G., & McCombs, J. (2016). Outcomes Associated With Primary and Secondary Nonadherence to Cholesterol Medications. AJPB® Translating Evidence-Based Research Into Value-Based Decisions®, 8(2). https://www.pharmacytimes.com/view/outcomes-associated-with-primary-and-secondary-nonadherence-to-cholesterol-medications
7. Iuga, A. O., & McGuire, M. J. (2014). Adherence and health care costs. Risk Management and Healthcare Policy, 7, 35–44. https://doi.org/10.2147/RMHP.S19801
8. Wells, A. (2022, March 14). Prescription Drug Prices No Longer the Fastest-Growing Medical Good or Service. GoodRx. https://www.goodrx.com/healthcare-access/drug-cost-and-savings/prescription-drugs-rise-faster-than-medical-goods-or-services
9. Cohen, R., Martin, E., de La Rocque, F., Thollot, F., Pecquet, S., Werner, A., Boucherat, M., Varon, E., Bingen, E., & Levy, C. (2013). Probiotics and Prebiotics in Preventing Episodes of Acute Otitis Media in High-risk Children: A Randomized, Double-blind, Placebo-controlled Study. The Pediatric Infectious Disease Journal, 32(8), 810–814. https://doi.org/10.1097/INF.0b013e31828df4f3
10. Alexander, G. C., Casalino, L. P., & Meltzer, D. O. (2003). Patient-Physician Communication About Out-of-Pocket Costs. JAMA, 290(7), 953–958. https://doi.org/10.1001/jama.290.7.953
11. Choudhry, N. K., Denberg, T. D., & Qaseem, A. (2016). Improving Adherence to Therapy and Clinical Outcomes While Containing Costs: Opportunities From the Greater Use of Generic Medications: Best Practice Advice From the Clinical Guidelines Committee of the American College of Physicians. Annals of Internal Medicine, 164(1), 41–49. https://doi.org/10.7326/M14-2427
12. Deafness and hearing loss. (n.d.). World Health Organization. Retrieved November 1, 2022, from https://www.who.int/health-topics/hearing-loss
13. Chien, W., & Lin, F. R. (2012). Prevalence of Hearing Aid Use Among Older Adults in the United States. Archives of Internal Medicine, 172(3), 292–293. https://doi.org/10.1001/archinternmed.2011.1408





